Overview
HIV co-infection is the most critical risk factor for the reactivation of latent tuberculosis (TB) infection (LTBI). Our recent work in macaques coinfected with Mtb/ SIV suggests that cytopathic effects of SIV resulting in chronic immune activation and dysregulation of T cell homeostasis correlate with reactivation of LTBI. Our lab builds on compelling data that the reactivation of LTBI during HIV co-infection is likely to be driven by the events of HIV replication and therefore focuses on the need to have optimum translational interventions directed at reactivation due to co-infection.
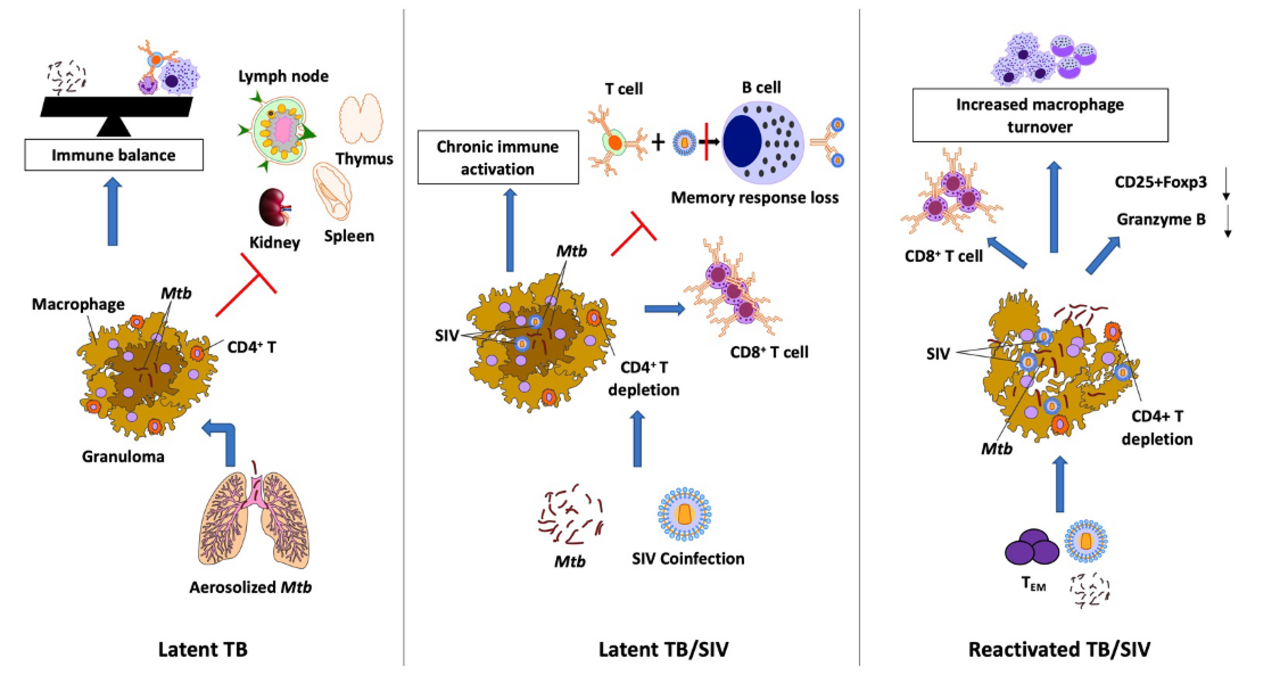
LTBI is characterized by a dynamic balance between the pathogen and the host as a consequence of limited bacterial replication due to its containment within granulomas. In the latent phase, the replication is contained in the granuloma by the activated T lymphocytes and macrophages. This leads to an arrest of the disease progression and an immune balance is attained. Co-infection with SIV leads to severe immunosuppression and as a result, there is an increase in the number of CD8+ T cells with increased expression of activation markers, CD95, CD38, and HLA-DR. Together, SIV co-infection with Mtb leads to chronic immune activation, immune dysbiosis, and a skewed Treg/TH17 balance resulting in reactivation of LTBI. Following the SIV-induced immune perturbation, there is a reduction in the generation of lung-homing Mtb-specific TEM CD4+ T cells. This preferred depletion of Mtb-specific CD4+ T cells and viral infection of the macrophages in the granulomas causes the integrity of the granuloma to disintegrate, leaking the contained Mtb and leading to dissemination.